11.7 Disorders of the Skeletal System
Created by CK-12 Foundation/Adapted by Christine Miller

Dowager’s Hump
The woman on the right in Figure 11.7.1 has a deformity in her back commonly called dowager’s (widow’s) hump, because it occurs most often in elderly women. Its medical name is kyphosis, and it is defined as excessive curvature of the spinal column in the thoracic region. The curvature generally results from fractures of thoracic vertebrae. As the inset drawings suggest, these fractures may occur due to a significant decrease in bone mass, which is called osteoporosis. Osteoporosis is one of the most prevalent disorders of the skeletal system.
Common Skeletal System Disorders
A number of disorders affect the skeletal system, including bone fractures and bone cancers. However, the two most common disorders of the skeletal system are osteoporosis and osteoarthritis. At least ten million people in the United States have osteoporosis, and more than eight million of them are women. Osteoarthritis is even more common, affecting almost 1.4 million people in Canada, and 1 in 4 women over the age of 50. Because osteoporosis and osteoarthritis are so common, they are the focus of this section. These two disorders are also good examples to illustrate the structure and function of the skeletal system.
Osteoporosis
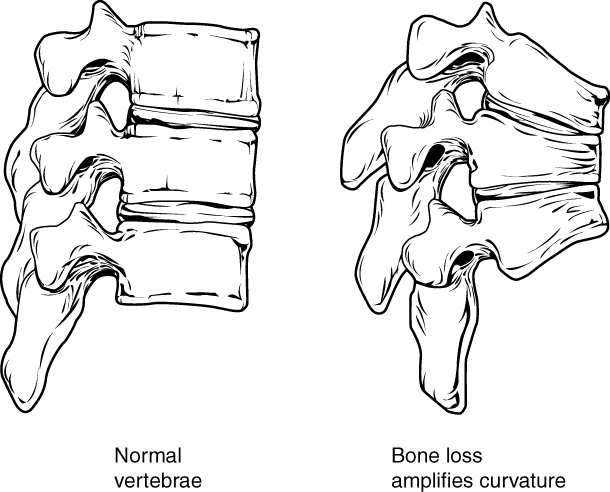
Osteoporosis is an age-related disorder in which bones lose mass, weaken, and break more easily than normal bones. Bones may weaken so much that a fracture can occur with minor stress — or even spontaneously, without any stress at all. Osteoporosis is the most common cause of broken bones in the elderly, but until a bone fracture occurs, it typically causes no symptoms. The bones that break most often include those in the wrist, hip, shoulder, and spine. When the thoracic vertebrae are affected, there can be a gradual collapse of the vertebrae due to compression fractures, as shown in Figure 11.7.2. This is what causes kyphosis, as pictured above in Figure 11.7.1.
Changes in Bone Mass with Age
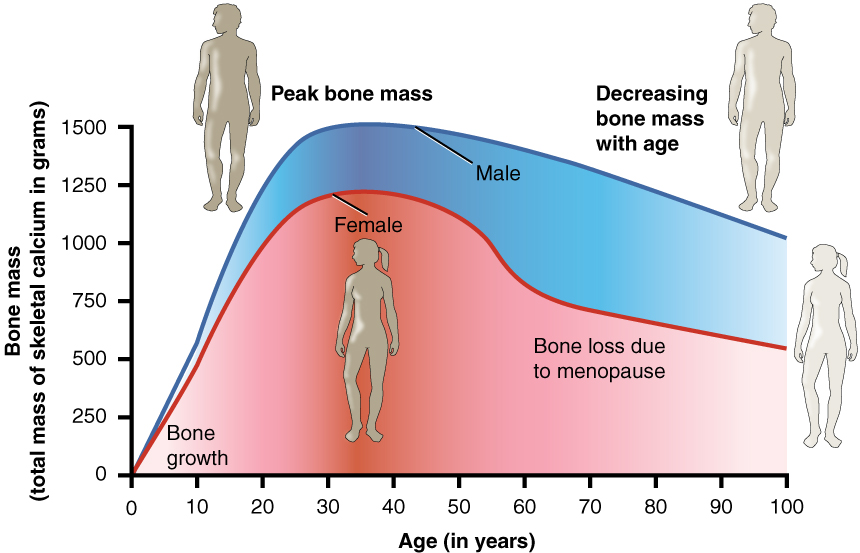
As shown in the Figure 11.7.3, bone mass in both males and females generally peaks when people are in their thirties, with males typically attaining a higher peak mass than females. In both sexes, bone mass usually decreases after that, and this tends to occur more rapidly in females, especially after menopause. The greater decrease in females is generally attributable to low levels of estrogen in the post-menopausal years.
What Causes Osteoporosis?
The underlying mechanism in all cases of osteoporosis is an imbalance between bone formation by osteoblasts and bone resorption by osteoclasts. Normally, bones are constantly being remodeled by these two processes, with up to ten per cent of all bone mass undergoing remodeling at any point in time. As long as these two processes are in balance, no net loss of bone occurs. There are three main ways that an imbalance between bone formation and bone resorption can occur and lead to a net loss of bone. All three ways may occur in the same individual. The three ways are described below:
- An individual never develops normal peak bone mass during the young adult years: If the peak level is lower than normal, then there is less bone mass to begin with, making osteoporosis more likely to develop.
- There is greater than normal bone resorption: Bone resorption normally increases after peak bone mass is reached, but age-related bone resorption may be greater than normal for a variety of reasons. One possible reason is calcium or vitamin D deficiency, which causes the parathyroid gland to release PTH, the hormone that promotes resorption by osteoclasts.
- There is inadequate formation of new bone by osteoblasts during remodeling: Lack of estrogen may decrease the normal deposition of new bone. Inadequate levels of calcium and vitamin D also lead to impaired bone formation by osteoblasts.
An imbalance between bone building and bone destruction leading to bone loss may also occur as a side effect of other disorders. For example, people with alcoholism, anorexia nervosa, or hyperthyroidism have an increased rate of bone loss. Some medications — including anti-seizure medications, chemotherapy drugs, steroid medications, and some antidepressants — also increase the rate of bone loss.
Diagnosing Osteoporosis
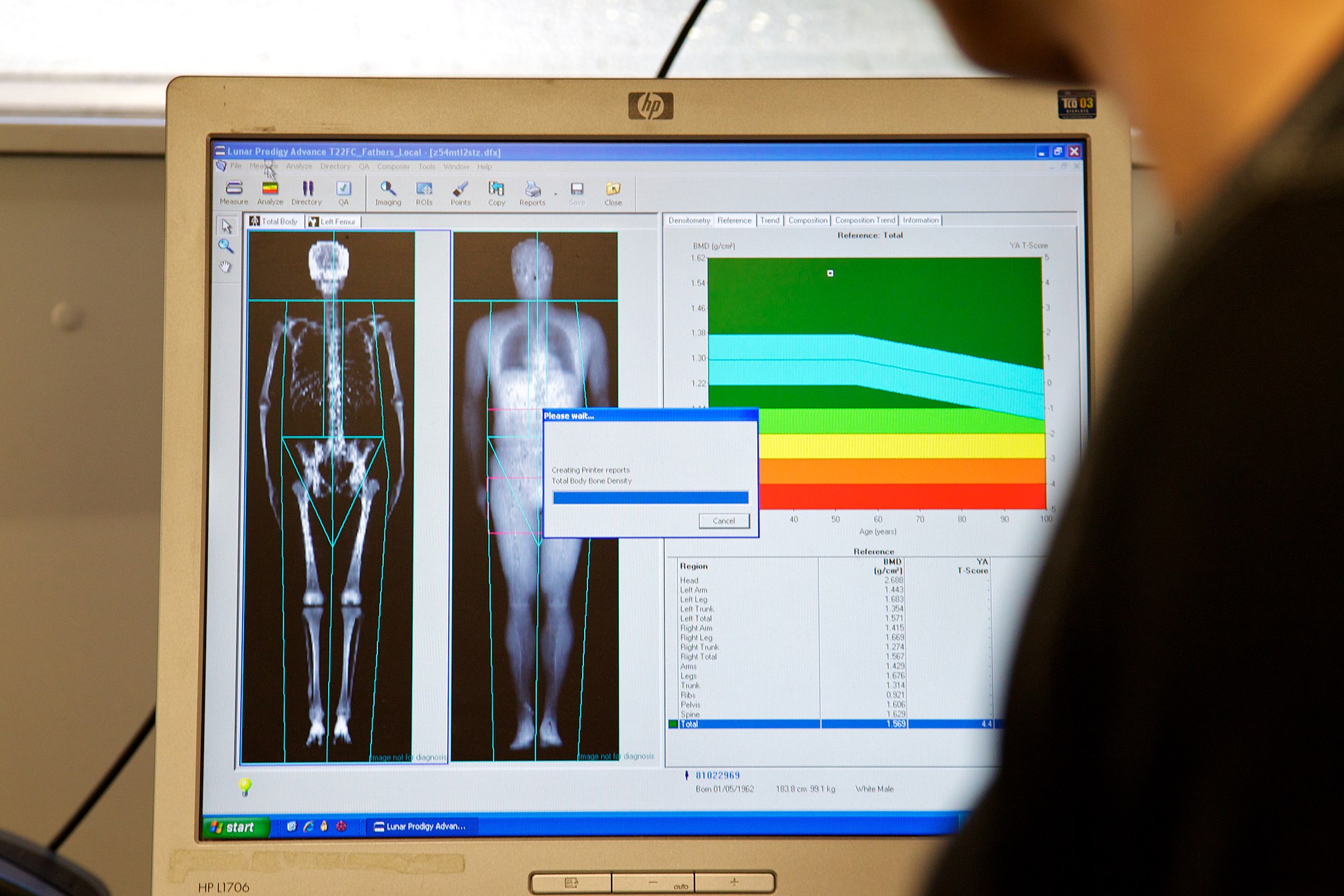
Osteoporosis is diagnosed by measuring a patient’s bone density and comparing it with the normal level of peak bone density in a young adult reference population of the same sex as the patient. If the patient’s bone density is too far below the normal peak level (as measured by a statistic called a T-score), then osteoporosis is diagnosed. Bone density is usually measured by a type of X-ray called dual-energy X-ray absorptiometry (or DEXA), an example of which is shown in Figure 11.7.4. Typically, the density is measured at the hip. Sometimes, other areas are also measured, because there may be variation in bone density in different parts of the skeleton. Osteoporosis Canada recommends that all women 65 years of age and older be screened with DEXA for bone density. Screening may be recommended at younger ages in people with risk factors for osteoporosis (see Risk Factors for Osteoporosis below).
Osteoporotic Fractures
Fractures are the most dangerous aspect of osteoporosis, and osteoporosis is responsible for millions of fractures annually. Debilitating pain among the elderly is often caused by fractures from osteoporosis, and it can lead to further disability and early mortality. Fractures of the long bones (such as the femur) can impair mobility and may require surgery. Hip fracture usually requires immediate surgery, as well. The immobility associated with fractures — especially of the hip — increases the risk of deep vein thrombosis, pulmonary embolism, and pneumonia. Osteoporosis is rarely fatal, but these complications of fractures often are. Older people tend to have more falls than younger people, due to such factors as poor eyesight and balance problems, increasing their risk of fractures even more. The likelihood of falls can be reduced by removing obstacles and loose carpets or rugs in the living environment.
Risk Factors for Osteoporosis
There are a number of factors that increase the risk of osteoporosis. Eleven of them are listed below. The first five factors cannot be controlled, but the remaining factors generally can be controlled by changing behaviors.
- Older age
- Female sex
- European or Asian ancestry
- Family history of osteoporosis
- Short stature and small bones
- Smoking
- Alcohol consumption
- Lack of exercise
- Vitamin D deficiency
- Poor nutrition
- Consumption of soft drinks
Treatment and Prevention of Osteoporosis
Osteoporosis is often treated with medications that may slow or even reverse bone loss. Medications called bisphosphonates, for example, are commonly prescribed. Bisphosphonates slow down the breakdown of bone, allowing bone rebuilding during remodeling to keep pace. This helps maintain bone density and decreases the risk of fractures. The medications may be more effective in patients who have already broken bones than in those who have not, significantly reducing their risk of another fracture. Generally, patients are not recommended to stay on bisphosphonates for more than three or four years. There is no evidence for continued benefit after this time — in fact, there is a potential for adverse side effects.

Preventing osteoporosis includes eliminating any risk factors that can be controlled through changes of behavior. If you smoke, stop. If you drink, reduce your alcohol consumption — or cut it out altogether. Eat a nutritious diet and make sure you are getting adequate amounts of vitamin D. You should also avoid drinking carbonated beverages.
If you’re a couch potato, get involved in regular exercise. Aerobic, weight-bearing, and resistance exercises can all help maintain or increase bone mineral density (for example hiking as in Figure 11.7.5). Exercise puts stress on bones, which stimulates bone building. Good weight-bearing exercises for bone building include weight training, dancing, stair climbing, running, and hiking (see Figure 11.7.5). Biking and swimming are less beneficial, because they don’t stress the bones. Ideally, you should exercise for at least 30 minutes a day most days of the week.
Osteoarthritis (OA) is a joint disease that results from the breakdown of joint cartilage and bone. The most common symptoms are joint pain and stiffness. Other symptoms may include joint swelling and decreased range of motion. Initially, symptoms may occur only after exercise or prolonged activity, but over time, they may become constant, negatively affecting work and normal daily activities. As shown in Figure 11.7.6, the most commonly involved joints are those near the ends of the fingers, at the bases of the thumbs, and in the neck, lower back, hips, and knees. Often, joints on one side of the body are affected more than those on the other side.
What Causes Osteoarthritis?
OA is thought to be caused by mechanical stress on the joints with insufficient self-repair of cartilage. The stress may be exacerbated by low-grade inflammation of the joints, as cells lining the joint attempt to remove breakdown products from cartilage in the synovial space. OA develops over decades as stress and inflammation cause increasing loss of articular cartilage. Eventually, bones may have no cartilage to separate them, so bones rub against one another at joints. This damages the articular surfaces of the bones and contributes to the pain and other symptoms of OA. Because of the pain, movement may be curtailed, leading to loss of muscle, as well.
Diagnosing Osteoarthritis

Diagnosis of OA is typically made on the basis of signs and symptoms. Signs include joint deformities, such as bony nodules on the finger joints or bunions on the feet (as illustrated in Figure 11.7.7). Symptoms include joint pain and stiffness. The pain is usually described as a sharp ache or burning sensation, which may be in the muscles and tendons around the affected joints, as well as in the joints themselves. The pain is usually made worse by prolonged activity, and it typically improves with rest. Stiffness is most common when first arising in the morning, and it usually improves quickly as daily activities are undertaken.
X-rays or other tests are sometimes used to either support the diagnosis of OA or to rule out other disorders. Blood tests might be done, for example, to look for factors that indicate rheumatoid arthritis (RA), an autoimmune disease in which the immune system attacks the body’s joints. If these factors are not present in the blood, then RA is unlikely, and a diagnosis of OA is more likely to be correct.
Risk Factors for Osteoarthritis
Age is the chief risk factor for osteoarthritis. By age 65, as many as 80 per cent of all people have evidence of osteoarthritis. However, people are more likely to develop OA — especially at younger ages — if they have had a joint injury. A high school football player might have a bad knee injury that damages the joint, leading to OA in the knee by the time he is in his thirties. If people have joints that are misaligned due to congenital malformations or disease, they are also more likely to develop OA. Excess body weight is another factor that increases the risk of OA, because of the added stress it places on weight-bearing joints.
Researchers have found that people with a family history of OA have a heightened risk of developing the disorder, which suggests that genetic factors are also involved in OA. It is likely that many different genes are needed for normal cartilage and cartilage repair. If such genes are defective and cartilage is abnormal or not normally repaired, OA is more likely to result.
Treatment and Prevention of Osteoarthritis
OA cannot be cured, but the symptoms — especially the pain — can often be treated successfully to maintain good quality of life for people with OA. Treatments include exercise, efforts to decrease stress on joints, pain medications, and surgery.
Exercise
Exercise helps maintain joint mobility and also increases muscle strength. Stronger muscles may help keep the bones in joints correctly aligned, and this can reduce joint stress. Good exercises for OA include swimming, water aerobics (see Figure 11.7.8 below), and biking. These activities are recommended for OA, because they put relatively little stress on the joints.

Exercising in water provides buoyancy that places less stress on joints than the same exercises would on the ground or other hard surface.
De-stressing Joints
Efforts to decrease stress on joints include resting and using mobility devices such as canes, which reduce the weight placed on weight-bearing joints and also improve stability. In people who are overweight, losing weight may also reduce joint stress.
Pain Medications
The first type of pain medication likely to be prescribed for OA is acetaminophen (e.g., Tylenol). When taken as prescribed, it has a relatively low risk of serious side effects. If this medication is inadequate to relieve the pain, non-steroidal anti-inflammatory drugs (NSAIDs, such as ibuprofen) may be prescribed. NSAIDs, however, are more likely to cause serious side effects, such as gastrointestinal bleeding, elevated blood pressure, and increased risk of stroke. Opioids usually are reserved for patients who have suffered serious side effects or for whom other medications have failed to relieve pain. Due to the risk of addiction, only short-term use of opioids is generally recommended.
Surgery
Joint-replacement surgery is the most common treatment for serious OA in the knee or hip. In fact, knee and hip replacement surgeries are among the most common of all surgeries. Although they require a long period of healing and physical rehabilitation, the results are usually worth it. The replacement “parts” are usually pain-free and fully functional for at least a couple of decades. Quality, durability, and customization of artificial joints are constantly improving.
Try out this neat Virtual Hip Resurfacing activity by Edheads (you will need to enable Flash).
Feature: Myth vs. Reality
About one out of every 5 adults in Canada suffer from osteoarthritis. The more you know about this disease, the more you can do to avoid it or slow its progression. That means knowing the facts, rather than believing the myths about osteoarthritis.
Myth |
Reality |
| “Cracking my knuckles will cause osteoarthritis.” | Cracking your knuckles may lead to inflammation of your tendons, but it will not cause osteoarthritis. |
| “My diet has no effect on my joints.” | What and how much you eat does affect your body weight, and every pound you gain translates into an additional four pounds (or more!) of stress on your knees. Being overweight, therefore, increases the chances of developing osteoarthritis — and also the rate at which it progresses. |
| “Exercise causes osteoarthritis or makes it worse, so I should avoid it.” | This is one of the biggest myths about osteoarthritis. Low-impact exercise can actually lessen the pain and improve other symptoms of osteoarthritis. If you don’t have osteoarthritis, exercise can reduce your risk of developing it. Low-impact exercise helps keep the muscles around joints strong and flexible, so they can help stabilize and protect the joints. |
| “If my mom or dad has osteoarthritis, I will also develop it.” | It is true that you are more likely to develop osteoarthritis if a parent has it, but it isn’t a sure thing. There are several things you can do to decrease your risk, such as getting regular exercise and maintaining a healthy weight. |
| “Bad weather causes osteoarthritis.” | Weather conditions do not cause osteoarthritis, although in some people who already have osteoarthritis, bad weather seems to make the symptoms worse. It is primarily low barometric pressure that increases osteoarthritis pain, probably because it leads to greater pressure inside the joints relative to the outside air pressure. Some people think their osteoarthritis pain is worse in cold weather, but systematic studies have not found convincing evidence for this. |
| “Joint pain is unavoidable as you get older, so there is no need to see a doctor for it.” | Many people with osteoarthritis think there is nothing that can be done for the pain of osteoarthritis, or that surgery is the only treatment option. In reality, osteoarthritis symptoms often can be improved with a combination of exercise, weight loss, pain management techniques, and pain medications. If osteoarthritis pain interferes with daily life and lasts more than a few days, you should see your doctor. |
| “Osteoarthritis is inevitable in seniors.” |
Although many people over 65 develop osteoarthritis, there are many people who never develop it, no matter how old they live to be. You can reduce your risk of developing osteoarthritis in later life by protecting your joints throughout life. |
11.7 Summary
- A number of disorders affect the skeletal system, including bone fractures and bone cancers. The two most common disorders of the skeletal system are osteoporosis and osteoarthritis.
- Osteoporosis is an age-related disorder in which bones lose mass, weaken, and break more easily than normal bones. The underlying mechanism in all cases of osteoporosis is an imbalance between bone formation and bone resorption in bone remodeling. Osteoporosis may also occur as a side effect of other disorders or certain medications.
- Osteoporosis is diagnosed by measuring a patient’s bone density and comparing it with the normal level of peak bone density. Fractures are the most dangerous aspect of osteoporosis. Osteoporosis is rarely fatal, but complications of fractures often are.
- Risk factors for osteoporosis include older age, female sex, European or Asian ancestry, family history of osteoporosis, short stature and small bones, smoking, alcohol consumption, lack of exercise, vitamin D deficiency, poor nutrition, and consumption of soft drinks.
- Osteoporosis is often treated with medications — such as bisphosphonates — that may slow or even reverse bone loss. Preventing osteoporosis includes eliminating any risk factors that can be controlled through changes of behavior, such as undertaking weight-bearing exercise.
- Osteoarthritis (OA) is a joint disease that results from the breakdown of joint cartilage and bone. The most common symptoms are joint pain and stiffness. OA is thought to be caused by mechanical stress on the joints with insufficient self-repair of cartilage, coupled with low-grade inflammation of the joints.
- Diagnosis of OA is typically made on the basis of signs and symptoms, such as joint deformities, pain, and stiffness. X-rays or other tests are sometimes used to either support the diagnosis or rule out other disorders. Age is the chief risk factor for OA. Other risk factors include joint injury, excess body weight, and a family history of OA.
- OA cannot be cured, but the symptoms can often be treated successfully. Treatments may include exercise, efforts to decrease stress on joints, pain medications, and surgery to replace affected hip or knee joints.
11.7 Review Questions
- Create a brochure or poster about osteoporosis to educate others about this disease. Include information about:
- A definition of osteoporosis
- Causes
- Dangers of living with the disease
- Canadian osteoporosis statistics
- Risk factors
- Diagnosis
- Treatment
-
- Why is it important to build sufficient bone mass in your young adult years?
- Explain the difference in cause between rheumatoid arthritis and osteoarthritis.
- Debunk the myth: Osteoarthritis is caused by physical activity, so people who are equally active are equally susceptible to it.
- Explain how we know that estrogen generally promotes production of new bone.
11.7 Explore More
Kevin Stone: The bio-future of joint replacement, TED, 2010.
The benefits of good posture – Murat Dalkilinç, TED-Ed, 2015.
Attributions
Figure 11.7.1
Blausen_0686_Osteoporosis_01 by BruceBlaus on Wikimedia Commons is used under a CC BY 3.0 (https://creativecommons.org/licenses/by/3.0) license.
Figure 11.7.2
Feature_Osteoprosis_of_Spine by OpenStax College on Wikimedia Commons is used under a CC BY 3.0 (https://creativecommons.org/licenses/by/3.0) license.
Figure 11.7.3
Age_and_Bone_Mass by OpenStax College on Wikimedia Commons is used under a CC BY 3.0 (https://creativecommons.org/licenses/by/3.0) license.
Figure 11.7.4
DEXA_scan_screen_ALSPAC by Nick Smith photography on Wikimedia Commons is used under a CC BY-SA 3.0 license.
Figure 11.7.5
Hiking by jake-melara-Yh6K2eTr_FY [photo] by Jake Melara on Unsplash is used under the Unsplash License (https://unsplash.com/license).
Figure 11.7.6
Areas_affected_by_osteoarthritis by National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS)/ NIH on Wikimedia Commons is in the public domain (https://en.wikipedia.org/wiki/Public_domain).
Figure 11.7.7
Hallux_valgus by Malmstajn on Wikimedia Commons is used under a CC BY 3.0 (https://creativecommons.org/licenses/by/3.0) license.
Figure 11.7.8
07-06_WtrAerob1a by Tim Ross on Wikimedia Commons is in the public domain (https://en.wikipedia.org/wiki/Public_domain).
References
Betts, J. G., Young, K.A., Wise, J.A., Johnson, E., Poe, B., Kruse, D.H., Korol, O., Johnson, J.E., Womble, M., DeSaix, P. (2013, June 19). Figure 6.23 Graph showing relationship between age and bone mass digital image]. In Anatomy and Physiology (Section 6.6). OpenStax. https://openstax.org/books/anatomy-and-physiology/pages/6-6-exercise-nutrition-hormones-and-bone-tissue
Betts, J. G., Young, K.A., Wise, J.A., Johnson, E., Poe, B., Kruse, D.H., Korol, O., Johnson, J.E., Womble, M., DeSaix, P. (2013, June 19). Figure 7.22 Osteoporosis [digital image]. In Anatomy and Physiology (Section 7.3). OpenStax. https://openstax.org/books/anatomy-and-physiology/pages/7-3-the-vertebral-column
Blausen.com staff. (2014). Medical gallery of Blausen Medical 2014. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436.
Mayo Clinic Staff. (n.d.). Kyphosis [online article]. MayoClinic.org. https://www.mayoclinic.org/diseases-conditions/kyphosis/symptoms-causes/syc-20374205
Mayo Clinic Staff. (n.d.). Osteoarthritis [online article]. MayoClinic.org. https://www.mayoclinic.org/diseases-conditions/osteoarthritis/symptoms-causes/syc-20351925
TED. (2010, July 23). Kevin Stone: The bio-future of joint replacement. YouTube. https://youtu.be/DL0_gcP15Ts
TED-Ed. (2015, July 30). The benefits of good posture – Murat Dalkilinç. YouTube. https://www.youtube.com/watch?v=OyK0oE5rwFY&feature=youtu.be
Wheatley, G., Smail, S., Bort, E. (2007). Virtual hip resurfacing [online game]. EdHeads.org. https://edheads.org/page/hip_resurfacing
A medical condition in which the bones become brittle and fragile from loss of tissue, typically as a result of hormonal changes, or deficiency of calcium or vitamin D.
The degeneration of joint cartilage and the underlying bone, most common from middle age onward. It causes pain and stiffness, especially in the hip, knee, and thumb joints.
A type of bone cell that makes and mineralizes bone matrix.
A type of bone cell that breaks down bone, dissolves its minerals, and releases them into the blood.
The compulsive use of a drug, despite negative consequences that such use may entail.
The body system composed of bones and cartilage and performs the following critical functions for the human body: supports the body. The skeletal system facilitates movement, protects internal organs, and produces blood cells.
A group of diseases involving abnormal cell growth with the potential to invade or spread to other parts of the body.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}